Treatment
Some patients my undergo one or more of this therapies in the management of their Disease, but surgery remains the primary treatment for rectal cancer. local therapy or systemic therapy. Treatment could be either by Local therapies which consist of surgery, radiation therapy and interventional radiology. These therapies can remove or destroy cancer in a particular area of the body such as the colon, rectum, liver, lungs, peritoneum, etc. The other is by Systemic therapy consists of chemotherapy and biological therapy, for these drugs enter the bloodstream and destroy or control cancer throughout the body. Surgeries can be categorized into curative, palliative, bypass, fecal diversion, or open and close performed with instruments that can be placed directly into the rectum from the anus or by incision of the lower abdominal skin (incision).
Curative: Surgical treatment can be offered with intention of curing the patient completely from the tumor, this could be done in early cancer stage (Stage 0 and I) by removing the polyp at the time of colonoscopy. Surgeries include the total mesorectal excision (lower anterior resection) or abdominoperineal excision (Both discussed below).
If distant metastases are present in a single organ (either the liver or lungs) and is small size and number, then curative surgery may also be possible as chemotherapy is given before and /or after the surgery to shrink before surgery or kill the remaining tumor after surgery thereby increasing survival rate of such patients.
Palliative: This is a non-curative surgery of the primary tumor for patients with a stage IV rectal cancer. This surgery is done for the purpose of reducing further symptom pain caused by tumor, mostly to stop bleeding and invasion as Chemotherapy and Radiation are just the main treatment.
Bypass: This is a surgery done if the tumor invaded into structures around the rectum making surgery technically difficult, the surgeons may prefer to completely cut of the whole or part of effected rectum then reattaching the remaining part to the anal canal or to the abdominal wall. This whole procedure is for fecal diversion which refers to the surgical creation of an anastomosis or colostomy.
Open and Close Surgery: This is in the case when surgeons have an abdominal incision to make a bypass but find the tumor extending to the small intestine making it impossible for any action to be taken. Any more procedures would do more harm than good to the patient. Note: This is uncommon with the advent of laparoscopy and better radiological imaging. Most of these cases formerly subjected to “open and close” procedures are now diagnosed in advance and surgery avoided.

Fig8.2 Diagram representation of a colostomy@ Ntional cancer institute
Stage 0 and Stage I Surgery include
1. Polypectomy (stage 0) and Local Excision (Early Stage I)
Polyps can be removed by surgery through a colonoscope as discussed in the examination chapter. Early stage (stage I) cancers lining the mucosa can be removed along with a small amount of nearby tissue. Local excision removes superfical cancers and a small amount of nearby tissues. This can be done with instruments inserted through the anus without making a surgical incision on the abdominal skin as shown in fig9.1 below.
2. Local Transanal Resection - Full Thickness Resection (Stage I Cancers)
This procedure is similar to procedure above, via the anus but it involves cutting through all layers of the rectum to remove cancer as well as some surrounding normal rectal tissue. This procedure can be used to remove some stage I (fig9.0B) rectal cancers that are relatively small and not too far from the anus.
3. Transanal Endoscopic Microsurgery – TEM (Stage I Cancers)
This operation can sometimes be used for early stage cancers that are higher in the rectum than could be reached using the standard transanal resection. A specially designed microscope is placed through the anus, allowing the surgeon to do a transanal resection with great precision and accuracy. This operation is only done at certain centers, as it requires special equipment and surgeons with special training and experience.

fig9.0A Illustration of Stage0 Cancer© 2010, Saint Francis Care
|

fig9.0B Illustration of stage II cancer © 2010, Saint Francis Care
|
Note: Colostomy is a procedure of colon or rectum is removed, but reconnection becomes impossible. In this case, the surgeon creates a new path for waste to leave the body via the the wall of the abdomen.
Stage II and III Surgery:
These surgeries may also be undertaken by a stage I patient depending on the Doctors advice.
1. Low Anterior Resection (Some Stage I, Most Stage II or III)
This procedure is done on Patients with cancers in the upper third of the rectum (close to where it connects with the colon).Patients will most likely be instructed to take laxatives and enemas before surgery to completely clean out the intestines. Just before surgery, the patient will be given general anesthesia, which puts them into a deep sleep. Incision is done on the lower abdominal wall to cut off the part effected, the colon is then re-attached to the remaining part of the rectum with a normal fecal movement to the anus. If radiation and chemotherapy have been given before surgery (neoadjuvant), it is common for a temporary colostomy to be made (where the last part of the colon is brought out through a hole in the abdominal wall). Usually this can be closed about 8 weeks later. The usual hospital stay for a low anterior resection is 4 to 7 days, depending on the patient’s overall health. Recovery time at home may be 3 to 6 weeks.
2. Proctectomy with Colo-Anal Anastomosis (Some Stage I, Most Stage II and III Cancers)
This procedure is similar to the last one but has a different case situation, where the cancer affects the middle and lower third of the rectum. This will require removal of the entire rectum (proctectomy) and the colon then attached to the anus in a procedure called colo-anal connection (anastomosis). Removal of the rectum is necessary, which is required to remove all of the lymph nodes near the rectum this is called total mesorectal excision (TME). This is a harder procedure to do but modern techniques have made it possible. Sometimes when a colo-anal anastomosis is done, a small pouch is made by doubling back a short segment of colon (colonic J-pouch) . This small reservoir of colon then functions as a storage space for fecal matter like the rectum did before surgery. Special technique is done to avoid a permanent colostomy, by performing a temporary colostomy as seen in fig8.2 opening for about 8 weeks while the bowel heals. A second operation is then performed to close the colostomy opening. The usual hospital stay for a colo-anal anastomosis, like a low anterior resection, is 4 to 7 days, depending on the patient’s overall health. Recovery time at home may be 3 to 6 weeks.
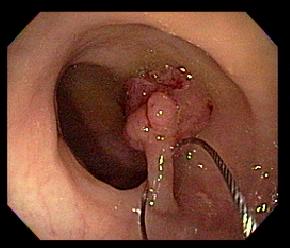
Fig9.1 Diagram Illustrating technique of endoscopic polypectomy @colorectal-cancer.ca
|
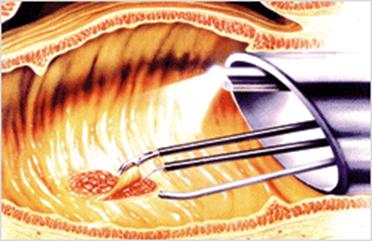
Fig9.1B Diagram Illustrating Transanal Endoscopic Microsurgery Removing Rectal [email protected]
|
3. Abdominoperineal Resection (Some Stage I, Most Stage II or III Cancers)
A procedure for cancers in the lower third of the rectum (the part nearest to the anus), especially if the cancer is growing into the sphincter muscle (the muscle that keeps the anus closed and prevents stool leakage). Here, the surgeon makes one incision in the abdomen and another in the perineal area around the anus. The incision in the perineal area incision allows the surgeon to remove the anus and the tissues surrounding it, including the sphincter muscle.While the incision on the abdomen is for the surgeon to section part of the rectum unaffected and attached it to the abdominal wall for permanent colostomy because the anus is removed, this is to allow stool a path out of the body. The usual hospital stay for an abdominoperineal resection is 4 to 7 days, depending on the overall health of the patient. Recovery time at home may be 3 to 6 weeks.
4. Total Mesorectal Excision (Stage II and III)
Total mesorectal excision (TME) was described 20 years ago and is now being established as the therapeutic gold standard for middle and lower third rectal cancers in a number of countries worldwide, including Canada.The mesorectum is a fatty tissue directly adjacent to the rectum that contains blood vessels and lymph nodes. When rectal cancers recur, it is often in these lymph nodes. In a TME surgery, surgeons carefully remove the entire mesorectum and lymph nodes, leading to a very low risk that cancer will recur in the local region. TME surgery sometimes impairs rectal function and results in patients requiring a permanent colostomy. Although the risk is never eliminated, having the surgery performed by an experienced physician can make this outcome less likely. Following surgery, patients sometimes also receive radiation and/or chemotherapy and the same can be said before the surgery as well. Combining chemotherapy and radiation either before or after TME is yielding promising long term results and a low risk for local recurrence. Patients who have rectal cancer that is confined to the lower two-thirds of the rectum are generally considered good candidates for TME surgery. However, many factors can determine whether TME is appropriate for the patient and should therefore be discussed with the patient’s surgeon.
In a total mesorectal excision, the surgeon cuts away the piece of rectum with the cancer, some tissue above and below it, and the layer of fatty tissue around the rectum. As previously state, this layer of tissue is called the mesorectum, which is made up of fat, blood vessels, and lymph tubes, and it is closely stuck to the rectum. The surgery aims to catch cancer cells that may have spread outside the wall of the rectum. This reduces the chances that the cancer will return. It also removes lymph nodes in the fatty layer. Older types of surgery do not take away the fatty layer. After the piece of rectum and the mesorectal tissue are removed, the two ends of the bowel that are left are joined back together. The procedure is usually done through one large cut. But some physicians are performing it using several smaller cuts and a camera to guide them (laparoscopic, or keyhole surgery) as illustrated in fig9.3. The research to date indicates that both operations work equally well. Recovery time from a keyhole operation appears to be quicker.
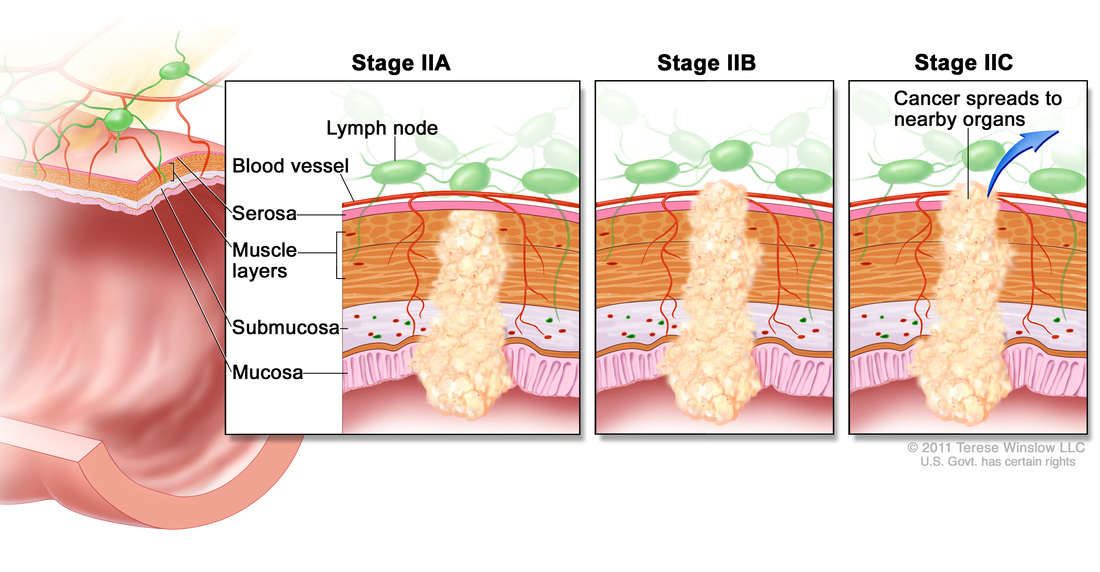
fig9.2A illustration of the various extend of stage II © 2010, Saint Francis Care
|

fig9.2B illustration of the various extend of stage III © 2010, Saint Francis Care
|
Note: After having had a TME, the frequency of bowel movements increases approximately two fold than if other types of surgery had been employed.
5. Pelvic Exenteration (Stage II, III & IV)
If the rectal cancer is growing into nearby organs, a pelvic exenteration may be recommended. This is an extensive operation. Not only will the surgeon remove the rectum, but also nearby organs such as the bladder, prostate (in men), or uterus (in women) if the cancer has spread to these organs. You will need a colostomy after pelvic exenteration. If the bladder is removed, you will also need a urostomy (opening where urine exits the front of the abdomen and is held in a portable pouch).
Side Effect of Rectal Surgery
Potential side effects of rectal surgery depend on several factors, including the extent of the operation and a person’s general health before surgery. Most people will have at least some pain after the operation, although this can usually be controlled with medicines if needed. Eating problems usually resolve within a few days of surgery. Other problems may include bleeding from the surgery, blood clots in the legs, and damage to nearby organs during the operation. Rarely, the connections between the ends of the intestine may not hold together completely and may leak, which can lead to infection. It is also possible that the incision might open up, causing an open wound. After the surgery, the patient might develop scar tissue that causes tissues in the abdomen to stick together called adhesions. In some cases, adhesions may cause the bowel to become blocked, requiring further surgery. Complications are rare but should be made aware to patients prior to surgery and generally they include:
5. Pelvic Exenteration (Stage II, III & IV)
If the rectal cancer is growing into nearby organs, a pelvic exenteration may be recommended. This is an extensive operation. Not only will the surgeon remove the rectum, but also nearby organs such as the bladder, prostate (in men), or uterus (in women) if the cancer has spread to these organs. You will need a colostomy after pelvic exenteration. If the bladder is removed, you will also need a urostomy (opening where urine exits the front of the abdomen and is held in a portable pouch).
Side Effect of Rectal Surgery
Potential side effects of rectal surgery depend on several factors, including the extent of the operation and a person’s general health before surgery. Most people will have at least some pain after the operation, although this can usually be controlled with medicines if needed. Eating problems usually resolve within a few days of surgery. Other problems may include bleeding from the surgery, blood clots in the legs, and damage to nearby organs during the operation. Rarely, the connections between the ends of the intestine may not hold together completely and may leak, which can lead to infection. It is also possible that the incision might open up, causing an open wound. After the surgery, the patient might develop scar tissue that causes tissues in the abdomen to stick together called adhesions. In some cases, adhesions may cause the bowel to become blocked, requiring further surgery. Complications are rare but should be made aware to patients prior to surgery and generally they include:
- Sexual dysfunction
- Irregular bowel movements
- Gas and flatulence
- Diarrhea
- Bladder complications
- Sense of urinary urgency
- Fecal incontinence
- Complications in or around the abdominal for colostomy, if one is created
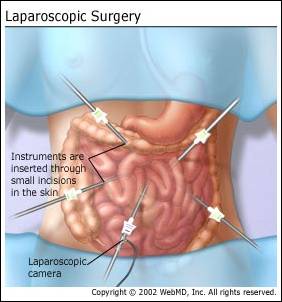
Fig9.3 Laproscopy a minimally invasive technique @colorectal-cancer.ca
copyright@2013 K.Bobbo
